Chronic kidney disease affects hundreds of thousands of Washingtonians, yet most remain undiagnosed until the disease has progressed to a late, costly stage. Washington Health Alliance identified CKD as a high-priority opportunity for collaborative action: a condition where earlier diagnosis and evidence-based treatment can meaningfully reduce harm to patients and costs to employers and health plans. Beginning in 2023, WHA developed a strategic plan to build and engage a coalition of providers, health plans, employers, and community organizations with the will and the tools to shift CKD care upstream.
Coalition-building began with a September 2023 webinar, followed by a health plan medical director roundtable in September 2024 and a provider and community organization workgroup in October 2024. Both convenings surfaced concrete, high-impact opportunities for plans and providers to improve their processes, and participants called for a formal CKD Learning Collaborative in Washington modeled on the National Kidney Foundation's approach.
In 2025, with support from Bayer and Boehringer Ingelheim, WHA developed a new set of claims-based CKD measures grounded in national care guidelines. Those measures went through rigorous internal vetting, and from that foundation WHA launched a Learning Collaborative bringing together employers, health plan leaders, and clinicians to build action plans for improving early screening and treatment across Washington state.
WHA Releases CKD Dashboard on Community Checkup
Washington's CKD data is now public.
For the first time, health plans, employers, clinicians, and community organizations can see how well Washington identifies and treats chronic kidney disease before it reaches a late, costly stage. Eight new claims-based measures, built and vetted by WHA's multi-stakeholder coalition, are live on the Community Checkup. See where Washington stands and where the opportunity is.
Why Washington Health Alliance Is Leading the Way on Chronic Kidney Disease
Chronic kidney disease affects roughly 15% of American adults. Most don't know they have it. That's not a coincidence. It's a gap, and it's exactly the kind of gap Washington Health Alliance was built to close.
WHA chose this work because we knew it would make a real difference for our members. The data pointed clearly to an opportunity, and we have the tools, the relationships, and the reach to act on it. The result is what we believe is the first CKD quality measure reporting capability grounded in a voluntary All-Payer Claims Database, built with clinical experts, and designed to serve the people who need it most.
Chronic Kidney Disease
- About 15% of American adults have CKD, and most don't know it.
- 1 in 3 adults with diabetes has CKD.
- Diabetes drives 47% of CKD cases that progress to dialysis or transplant.
- Early-stage management costs roughly $7,725 over four months; a single heart failure hospitalization runs $31,063.
Read more
A Condition That Hides Until It Doesn't
CKD progresses quietly, with symptoms that are vague and easy to miss until the disease has already advanced.
The connection to conditions WHA already tracks makes this even more urgent. One in three adults with diabetes has CKD. Diabetes drives 47% of all CKD cases that progress to dialysis or transplant, and CKD with type 2 diabetes accounts for roughly 39% of all end-stage renal disease. These are patients already in the healthcare system, with a clear opportunity for early intervention. But only if someone is measuring for it.
The Cost of Waiting Is Enormous
Early-stage CKD is manageable. Four-month management costs for Stage I and II run approximately $7,725. That number is real, but it pales beside what happens when CKD advances undetected.
Once a patient reaches Stage III or beyond, the costs climb fast. According to research published in AJMC, a myocardial infarction costs $21,016, a stroke $21,087, a heart failure hospitalization $31,063, and atrial fibrillation hospitalization $30,500, compared to $5,162 for those without CKD. End-stage renal disease requiring dialysis or transplant represents a fundamentally different level of cost and human burden.
Through early screening, diagnosis, and treatment, Washington can work toward cutting the kidney transplant list by 50% over the next 30 to 40 years. That's not aspirational. It's achievable.
Early Action Changes the Trajectory
The clinical tools already exist. Blood pressure control, reno-protective medications, and targeted lifestyle changes can meaningfully slow CKD progression when started early. The barrier isn't treatment. It's identification.
That's a measurement problem, and measurement is what WHA does well.
Washington Health Alliance Is Built for This Moment
For more than 20 years, WHA has translated complex claims data into trusted, useful insight for Washington's healthcare community. No other organization in this state does this work with the same depth, independence, or reach.
Our voluntary All-Payer Claims Database represents more than 4 million covered lives across Washington. That scale gives us a view of care patterns and gaps that no single payer or health system can see alone.
For CKD, we paired that data with clinical expertise, working with the National Kidney Foundation and clinicians from health systems across the state to build a validated measure set covering CKD screening, diagnosis, and treatment, alongside the comorbid conditions that travel with it: diabetes, hypertension, and cardiovascular disease.
Our members need this. We built something worthy of that trust.
What This Makes Possible
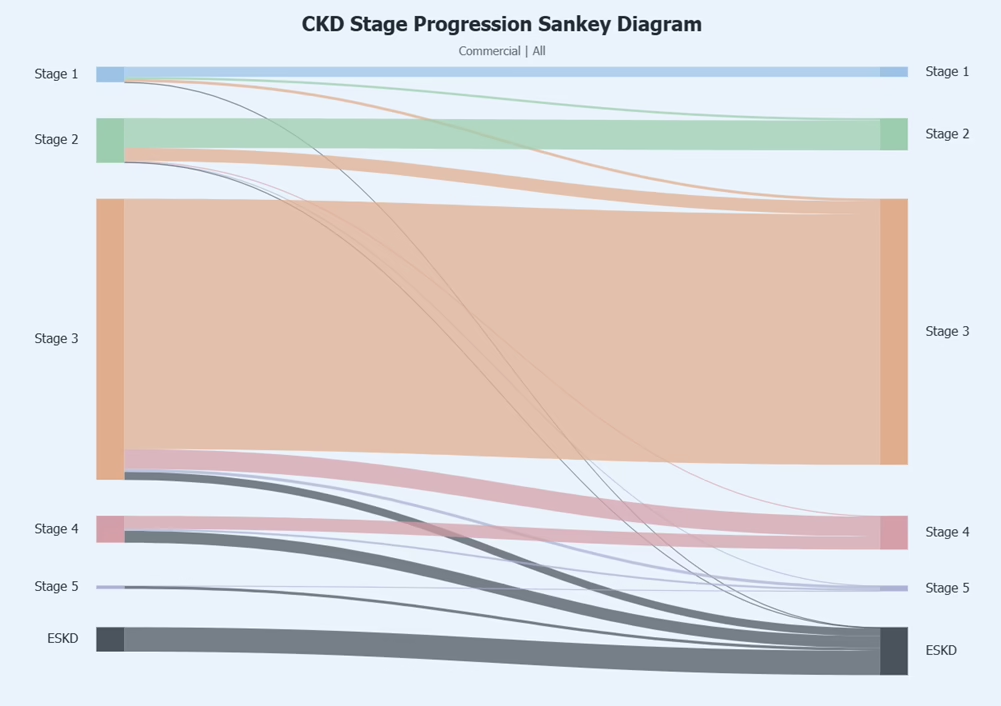
WHA's CKD dashboard brings together clinical staging, reno-protective medication use, disease progression, and end-stage renal disease endpoints, giving Washington's healthcare community the benchmarks it needs to see where care is strong and where it needs to improve.
We've already launched a learning collaborative with a dedicated group of members, translating these insights into better care for patients living with CKD.
WHA has always believed that better measurement leads to better care. With CKD, we have the chance to prove it at a scale that matters to every Washingtonian.
Read lessHow Washington Health Alliance Added the Capability to Measure Chronic Kidney Disease
Chronic kidney disease affects roughly 1 in 7 American adults. Most don't know they have it. That's not just a clinical problem. It's also a data problem. If we can't measure it, we can't improve it.
At Washington Health Alliance, we set out to change that. Drawing on more than 20 years of expertise in claims-based quality measures, we brought that foundation to a new challenge: our team developed what is, to our knowledge, the first-ever CKD quality measure reporting capability grounded in a voluntary All-Payer Claims Database (APCD) in Washington state. It was intensely iterative work, and the latest AI tools responsibly and meaningfully accelerated it. Here's how we did it, and what we learned along the way.
Read more
Starting with What Exists
We didn't reinvent the wheel. Before writing a single line of code, we reviewed condition definitions from NCQA, CMS, AHRQ, HHS, and other leading measure stewards to understand how CKD and related conditions are identified in claims-based reporting.
From there, we turned to clinical evidence. National guidelines from the American Diabetes Association, the American Heart Association, and KDIGO (Kidney Disease: Improving Global Outcomes) informed our metric expansion, particularly around hypertension management and reno-protective medications, two areas where the clinical evidence is strong and the claims data can track performance.
Building a Clinically Validated Measure Set
Claims data can tell you a lot, but only if you ask the right questions. Our Medical Director, Dr. Drew Oliveira, led a clinical review that brought in the National Kidney Foundation alongside practicing endocrinologists and nephrologists from multiple health systems across Washington state. The goal: pressure-test our measures against real clinical experience and confirm that what we tracked in the data reflected what clinicians need to know.
That review produced a measure set covering CKD screening, diagnosis, and treatment, including comorbid conditions that most commonly travel alongside CKD: diabetes, hypertension, and cardiovascular disease.
Mapping Disease States Across Millions of Records
Washington Health Alliance's APCD represents more than 4 million covered lives across the state. Turning that data into useful insight required reliable disease-mapping logic, the underlying rules that let us identify which members have CKD, which have related conditions, and where care gaps exist.
We built condition-mapping logic for each clinical state in the measure set, grounded in standardized value sets aligned with national definitions. This wasn't a one-time build; it required iteration, review, and refinement.
Using AI as a Tool, Not a Shortcut
Artificial intelligence played a meaningful role in this work, but always with human oversight built in. We used AI as a tool to support the underlying coding needed to match national clinical measures and prevalence metrics. Every iteration required analyst review and validation before anything moved forward.
We also used AI to scan the medical literature and confirm our results were consistent with prior published studies, especially relevant when working with claims-based datasets, which have known limitations compared to clinical records. AI helped us work faster. It didn't replace judgment.
Building for Transparency and Trust
One of our most important decisions was building an audit trail from final measure results back to the underlying clinical evidence. That traceability makes our results reviewable and defensible, critical for a measure set that health systems and payers can rely on to understand performance and drive improvement.
Under the hood, we built a structured data system designed to be modular and reusable, so the same foundational logic can power multiple measures without rebuilding from scratch each time. Each measure has its own evidence layer, and the whole system is designed to grow as our CKD work expands.
What Comes Next
This capability is a foundation, not a finish line.
The measures give Washington's healthcare community a new lens on how well we identify and treat chronic kidney disease across the state. And we're not waiting to put them to work.
We've already engaged a small, dedicated group of members in a learning collaborative focused on improving care practices and, ultimately, outcomes for patients living with CKD. That work is underway now.
We're proud of the work, and more excited about what it makes possible.
Read lessWho Is Involved
Chronic kidney disease is one of Washington's most underdiagnosed conditions, and the costs, clinical and financial, fall on patients, employers, and health plans alike. Washington Health Alliance leads a structured Learning Collaborative to change that, building on a first-of-its-kind CKD claims-based measures dashboard released publicly in May 2026 and translating that data into coordinated action across the state.
The Learning Collaborative brings together eight organizations spanning the full care continuum: health plan leaders, clinicians, lab company representatives, and a purchaser. Meeting through the remainder of 2026, participants work to increase CKD screening rates among high-risk patients, improve diagnostic accuracy through evidence-based tools and workflows, expand appropriate early-stage treatment, and reduce the cardiovascular events that make late-stage CKD so costly.
Members commit to active participation in structured convenings, apply learnings within their own organizations, and contribute to a final report that spreads successful strategies across Washington state. This is not a study group, it is a working coalition with shared measures, shared goals, and accountability for results.
How the Work Came Together
September - Launched
WHA hosted its first CKD educational webinar, establishing the foundation for multi-stakeholder collaboration.
September - Health plans convened
WHA brought together health plan medical directors to identify high-impact opportunities for improving CKD screening and care management.
October - Providers commit
A provider and community organization workgroup produced concrete commitments around early detection, equity, and cross-sector collaboration.
Measures developed
With support from Bayer and Boehringer Ingelheim, WHA developed and vetted a first-of-its-kind set of claims-based CKD measures grounded in national care guidelines.
January - Learning Collaborative launched
Employers, health plan leaders, and clinicians came together to build action plans for improving early CKD screening and treatment across Washington state.
May - Measures released publicly
After final internal review and development, WHA's CKD measures were released publicly through the Community Checkup platform.